Laryngeal Mask Airway(Two way)/(Re-useable)
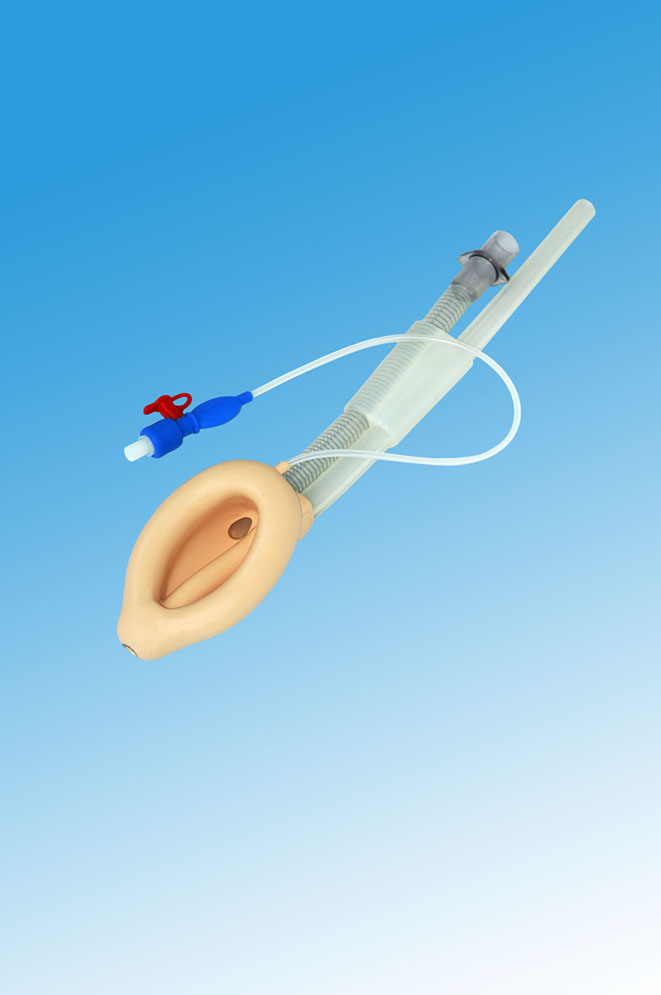
Laryngeal Mask is composed of 1. Drain tube orifice 2. Cuff 3. Rear boot 4 joint part 5. Drain tube 6 airway tube 7. Bite block 8. Connector 9. Inflation tube 10. Pilot balloon 11. Manual vent (only for reusable mask) 12 valve
The cuff, connector, airway tube and drain tube are integrated by gluing and so are the cuff, inflation tube and pilot balloon.
The valve and connector connect with pilot balloon and airway tube respectively through over-filling. There is an indicated marking line and maximum inflation volume mark on outer surface of airway tube. All components of Laryngeal Mask touching human body are made of silicone of medical degree.
Size |
ID of airway tube (mm) |
ID of Drain Tube (mm) |
Infaltion Volumn≤mL |
≤cm/H2O |
Applied Patient/Weight |
Connectot |
1.5 |
6 |
4.7 |
7 |
60 |
5 kg -10 kg |
ISO5356-1 15mm conical connector |
2.0 |
6.4 |
4.7 |
10 |
10 kg -20 kg |
2.5 |
7.5 |
6.0 |
14 |
20 kg -30 kg |
3.0 |
9.0 |
6.5 |
20 |
30 kg -50 kg |
4.0 |
9.0 |
6.5 |
30 |
50 kg -70 kg |
5.0 |
10.0 |
7.5 |
40 |
70kg -100kg |
RE-USEABLE SILICONE LARYNGEAL MASK

FEATURES:
- 100% medical-grade Dow Corning silicone.
- Abrasive-effect cuff; designed with aperture bars.
- Can be autoclaved repeatedly at 134 ℃ (deflate the cuff before sterilization).
- Reusable up to 40 times.
Size(#) |
Maximum Cuff Inflation Volumes(ml) |
Patient Weight(KG) |
1 |
4 |
0-5 |
1.5 |
7 |
5-10 |
2 |
10 |
10-20 |
2.5 |
14 |
20-30 |
3 |
20 |
30-50 |
4 |
30 |
50-70 |
5 |
40 |
70-100 |
Disposable Silicone Laryngeal Mask

Made of 100% medical grade silicone.
The cuff is made of medical grade silicone, and its specially designed shape coincides with the laryngopharynx well, reducing stimulation to patient body and improving the cuff seal.
Suitable for adult, children and infant use.
Size ( # ) |
Maximum Cuff Inflation Volumes (mL) |
Color Code |
Patient Weight(KG) |
Remark |
1 |
4 |
Flesh |
0-5 |
disposable |
1.5 |
7 |
Blue |
5-10 |
2 |
10 |
Green |
10-20 |
2.5 |
14 |
Orange |
20-30 |
3 |
20 |
Red |
30-50 |
4 |
30 |
Yellow |
50-70 |
5 |
40 |
Purple |
70-100 |